【English】What are Cleft Lips and a Cleft Palates? Prenatal Diagnosis and Treatment
What are Cleft Lips and a Cleft Palates? Prenatal Diagnosis and Treatment
Cleft lips and a cleft palates are both congenital defects in which a split occurs in the upper lip and upper jaw, respectively. Although they can be confirmed after birth, they have in recent years been detected increasingly by prenatal ultrasonographic screening before a baby is born. A child born with a cleft lip and/or cleft palate can, if given appropriate medical treatment, lead a social life comparable to that of a healthy individual.
What are cleft lips and cleft palates?
A baby
Courtesy of Payless Images
Defects in which a split occurs in the upper lip and upper jaw, respectively.
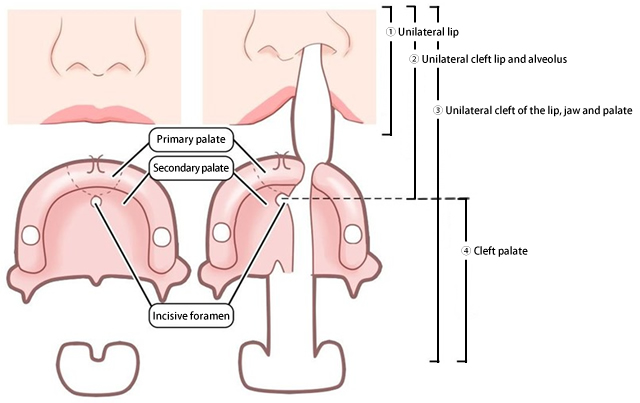
Both a cleft lip and a cleft palate are congenital diseases in which a split occurs in the labium (upper lip) and in the palate (upper jaw; the roof the mouth), respectively. Splits in the upper lip and upper jaw may appear on one or both sides of the mouth. Occasionally, splits may be seen from the nose to the back of the throat, and then to the uvula (a soft projection at the back of the throat).
Many classifications
Cleft lips and cleft palates are classified according to the type of split. They are basically classified into the following types.
- The upper lip has a split. (Cleft lip)
- The upper lip and upper gum have a split. (Cleft lip and alveolus)
- The upper lip, upper jaw, and uvula have a split. (Cleft lip and cleft palate)
- Only the upper jaw has a split. (Cleft palate)
What can be detected by ultrasonographic screening for a cleft lip and a cleft palate?
Echographic Screening
Courtesy of Payless Images
A cleft lip can generally be detected, but sometimes not
A cleft lip can sometimes be detected by prenatal fetal diagnosis. This is because echography* (ultrasonography) allows one images to be obtained of the shapes and characteristics of the baby's face.
If the echo is successfully delineated, features such as the positions of the eyes and the jaw will appear as they are, and it can be reasonably determined as to whether or not a cleft lip has occurred. However, the technique may not work well, depending on the scanning procedures and the posture of the baby.
* Echography is an imaging modality that visualizes reflected ultrasound waves and enables observation of the state of the mother's womb.
A cleft palate can rarely be diagnosed
A cleft palate cannot be detected by fetal diagnosis. This is because echographic imaging cannot display the inside of the baby's mouth. In particular, a cleft palate (splitting of the upper jaw) that has occurred alone cannot be detected by fetal diagnosis.
Often detected after 20 to 30 weeks of gestation
Echographic screening can detect cleft lip as early as 20 weeks into pregnancy. More often, however, it may not be noticeable until after 30 weeks.
Echocardiographic findings may differ from postnatal symptoms
A diagnosis of cleft lip or cleft palate is only definitive after birth. As mentioned earlier, not all abnormalities can be detected by echographic screening.
Echographic findings may differ from postnatal symptoms in the following cases:
- Echographic screening showed that one side of the mouth might have a split, but a bilateral cleft lip was confirmed after birth.
- Echographic screening revealed a split on one side of the mouth has a split, and a cleft palate was also found after birth.
What are cleft lips and cleft palates?
Family
Courtesy of Payless Images
Most cases are caused by multifactorial inheritance
Many cases of a cleft lip and a cleft palate are thought to result from genetic mutations (multifactorial inheritance) caused by genetic and environmental interactions. Multifactorial inheritance is a genetic phenomenon in which the appearance, shape, and constitution are expressed due to the influence of genetic factors and environmental factors (causes other than inheritance, such as lifestyle) rather than due to a single gene.
A cleft lip and/or cleft palate occurs in approximately 1 in 500 births
About one out of every 500 babies has a cleft lip and/or cleft palate.
The incidence of a cleft lip with or without a cleft palate is different from that of a cleft palate alone.
Recurrence rate varies from case to case
The recurrence rate of a cleft lip and a cleft palate (multiple cases in a family) differs depending on how many siblings have developed the defect and how many close relatives have been affected. It also depends on the morphological classification (types).
Treatment methods for a cleft lip and a cleft palate
Hospital
Courtesy of Payless Images
Treatment methods for a cleft lip and a cleft palate have been established
Cleft lip and cleft palate problems are mainly focused on facial features, speech and language, dental bite, and eustachian tube function (e.g., otitis media with effusion*). In most cases, treatment can improve the conditions so that no functional impairment remains.
Treatment for a cleft lip and a cleft palate is advancing more and more each day, and most patients with a cleft lip and/or cleft palate can, if they receive the appropriate treatment at the appropriate time, live a healthy social life comparable to that of a healthy person.
In particular, since the introduction of preoperative orthognathic treatment, which is used to shape the jaw prior to surgery, surgical methods have changed, and the number of surgeries required has been drastically reduced (the preoperative orthognathic treatment is described in detail below).
Treatment of a cleft lip and a cleft palate varies according to the medical institution. Here, we introduce the treatment methods being implemented by Kanagawa Children's Medical Center as of 2019.
For the treatment of a cleft lip and a cleft palate at the center, we have a team of experienced surgeons, including those certified by the Japan Society of Plastic and Reconstructive Surgery, who specialize in plastic surgery (the departments of neonatology, genetics, general medicine, otolaryngology, orthodontics, pediatric dentistry, and speech-language therapy), establishing a system that includes long-term follow-ups.
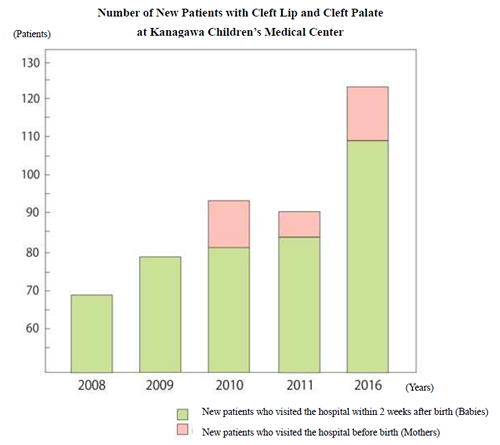
Incidence rate of new patients with cleft lip and/or cleft palate *
Otitis media with effusion is a condition in which fluid accumulates behind the eardrum membrane. Normally, the tensor veli palatini muscle, which adheres mainly to the eustachian tube (the tube connecting the nasal cavity and the middle ear), contracts and opens the eustachian tube to drain exudate from the nasal cavity. In the case of a cleft palate, the tensor veli palatini muscle is divided into right and left sides, which prevents the eustachian tube from opening, thereby allowing the exudate to pass from the nasal cavity to the middle ear. The condition in which the exudates accumulate is called "otitis media with effusion." If left untreated, otitis media with effusion may cause hearing loss, hence a baby with a cleft palate should be examined by an otolaryngologist around 6 months after birth, when the inside of the ears is more visible, and have an incision made in the eardrum membrane or surgery to insert a tube if necessary.
Treatment Schedules and Methods at Kanagawa Children's Medical Center
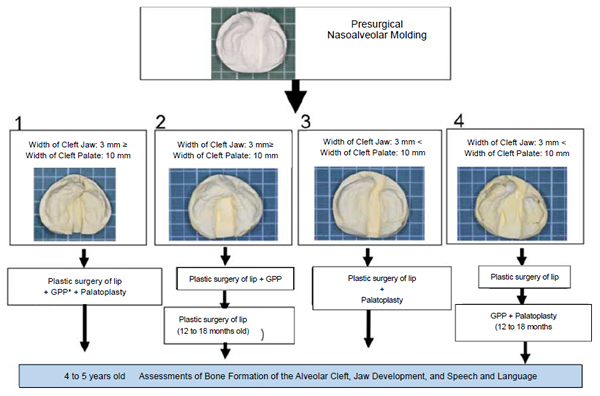
* GPP = gingivoperiosteoplasty: a type of surgery to close splits in the gums
Treatment protocols for unilateral cleft lips and cleft palates used in our department
I will talk about the treatment of cleft lips and cleft palates at this center in as detailed a manner as possible.
Main Schedules for Treatment of Cleft Lip and Cleft Palate
- Before birth: Informed consent (doctor's explanation and patient's consent) is obtained before birth from the parent whose baby is diagnosed as having a cleft lip and/or cleft palate.
- After birth: Preoperative jaw orthognathic treatment is performed, and general physical conditions are checked. (Our center has all the departments necessary for the treatment of cleft lip and cleft palate, including neonatology, genetics, general medicine, otolaryngology, orthodontics, and pediatric dentistry, each of which has experience in treating cleft lips and cleft palates).
- Cleft lip (the upper lip alone has a split): plastic surgery of the lip is performed using a minimal triangular flap technique around 3 to 4 months after birth.
- Cleft lip and alveolus (the upper lip and the gums have a split): presurgical nasoalveolar molding is performed as soon as possible after birth (if necessary), followed by plastic surgery of the lip.
- Cleft palate (the upper jaw alone has a split): palatoplasty using Furlow's technique and surgery for otitis media with effusion (if necessary) are performed around 1 year after birth.
- Cleft lip and cleft palate (the upper lip, upper jaw and uvula have a split): presurgical nasoalveolar molding is performed as soon as possible after birth, followed by the simultaneous procedures of plastic surgery of the lip with minimal triangular flap technique, GPP, palatoplasty with Furlow's technique, and surgery for otitis media with effusion (if necessary).
In the treatment of a cleft lip and a cleft palate, the timing of surgery and treatment sequences vary depending on the results of presurgical nasoalveolar molding treatment after birth. Multiple surgeries may be required, such as when the cleft lip and cleft palate is pronounced or when the child has an aversion to receive presurgical nasoalveolar molding treatment. In most patients, however, the swelling after surgery is minimal, and so the patient can be extubated (the respiratory tube is removed during anesthesia) and awakened soon after surgery.
What is Presurgical Nasoalveolar Molding Treatment?
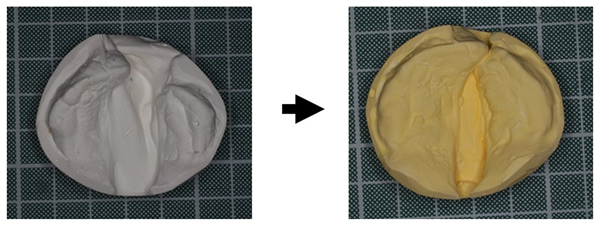
Plates used in presurgical nasoalveolar molding treatment:left:Before treatment; right:
After treatment
Presurgical nasoalveolar molding treatment is a preparation that is performed prior to surgery for cases involving pronounced clefts. Usually, plates and tapes are attached to narrow the cleft palate (cleft in the upper jaw). Plates and tapes remain in place until 5 to 6 months after birth. While wearing them, the patient needs to visit the hospital once every 10 to 14 days. When the cleft has been reduced by presurgical nasoalveolar molding treatment, surgery on the lip, jaw, and cleft palate can be performed.
What is plastic surgery of the lip using minimal triangular flap method?
Before suturing/After suturing
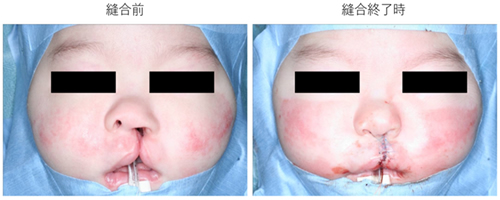
Plastic surgery of cleft lip using minimal triangular flap method
Plastic surgery of the lip is a surgery to close a cleft in the upper lip, which mainly includes Millard's technique, the small triangular flap method, and Fischer's technique.
The small triangular flap method has the disadvantage in that the triangular flap stands out. In order to resolve this drawback, we have devised and use a minimal triangular flap method in which the triangular flap is reduced to 2 mm or less.
What is GPP?
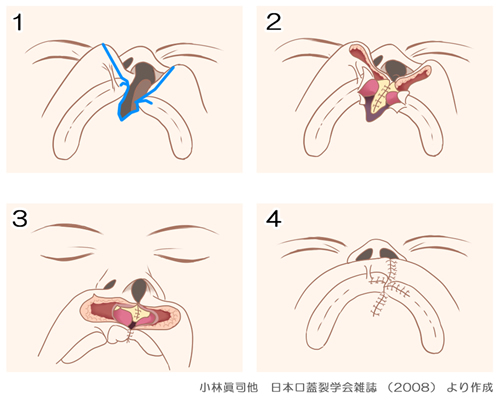
Created by Shinji Kobayashi, et al. Journal of Japanese Cleft Palate Association (2008)
Gingivoperiosteoplasty (GPP) is a surgical procedure to close clefts in the gums (where the teeth grow) during infancy. By peeling and suturing the mucoperiosteum surrounding the jaw with clefts, bone can be formed in a jaw having clefts. The ability to form bones is said to be very high during infancy. If this surgery is performed at the same time as the plastic surgery of the lip performed after birth, bone formation begins thereafter, so that there is no need for alveolar bone grafting (transplantation of iliac cancellous bone collected from the lumbar region to close the cleft in the gums during school age). Therefore, the number of surgeries can be reduced by one. Alveolar bone grafting is performed around the age of 6, because the iliac cancellous bone cannot be collected sufficiently it the patient is under 6 years old.
The gums are an important place as they are the foundations where permanent teeth will grow neatly arrayed in the future. The above treatment involves transplanting the patient's own bone (iliac cancellous bone) into the split gums (cleft jaw). For this reason, it is called "alveolar bone grafting." The treatment is usually performed between the ages of 6 and 10, when adequate iliac cancellous bone can be obtained and before the permanent teeth have emerged in the cleft.
As of 2019, insurance has also been applicable to the orthodontic treatment offered at our center and other accredited medical institutions. The combination of alveolar bone grafting and orthodontic treatment is an important part of the treatment of cleft lip and cleft palate. Needless to say, teeth are one of the important elements for staying healthy.
What is palatoplasty using Furlow's technique?
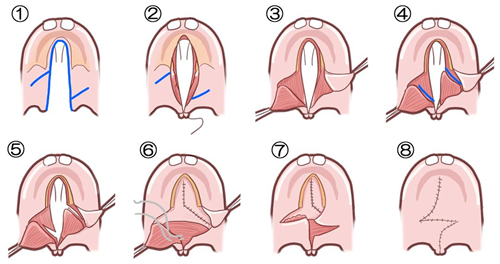
Suture in the order of 1 to 8 based on the Furlow's technique
A split in the roof of the mouth (palate) is called a cleft palate. Many people might think that a cleft lip and a cleft palate are defects that often cause lower jaw protrusion. However, neither a cleft lip nor a cleft palate always results in protruding upper jaw. Even though the jaw itself is normal, the growth of the upper jaw is inhibited, and so the lower jaw appears to protrude relatively. Upper jaw growth inhibition is generally considered to be often caused by surgery, especially palatoplasty, which is a procedure to treat a cleft palate in which the cleft runs from behind the teeth to the uvula.
Furlow's technique, a palatoplasty method, is considered to be a technique that can reduce growth inhibition of the jaw to as great an extent as possible, and is less likely to affect the patient's speech-language development.
A soft palate is treated with Z-plasty (an incision in a Z shape and stitching). For a hard palate, the mucoperiosteum is peeled and pulled toward the center to close the cleft.
In this way, all wounds can be covered with mucoperiosteum, and at the end of suturing, all of the sutures become linear scars. Furlow's technique covers all wounds with the patient's own mucoperiosteum, reducing the risk of upper jaw growth inhibition compared with other methods.
Before suturing/After suturing
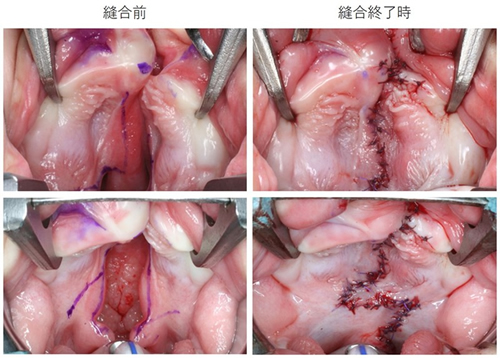
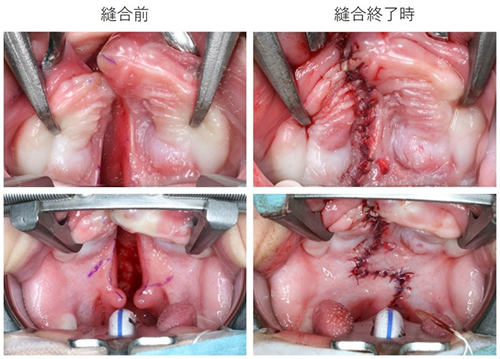
Before surgery/After performing Furlow's technique

A wide cleft palate can also be closed using Furlow's technique
Furlow's technique has been performed on a patient having a cleft palate with a wide split in the upper jaw. Orthodontic treatment will be performed from now own. The speech-language development (the way the patient speaks) is also good.
How can Furlow's technique close a wide cleft?
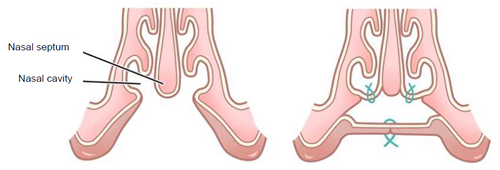
Cross-sectional views of the nasal cavity and cleft palate
A wide cleft palate can also be closed using height
Furlow's technique reduces upper growth inhibition and has beneficial effects on speech-language development. In general, however, Furlow's technique is not used for all cases with clefts of the palate. The greatest reason for this being that the technique cannot manage wider clefts.
We close a cleft hard palate by peeling the mucoperiosteum of the hard palate, which is one of the advantages of the Furlow's technique. A wide cleft palate can also be closed in this way.
Possible Symptoms after Surgery for Cleft Lip and Cleft Palate
Presurgical nasoalveolar molding treatment may increase the likelihood of upper jaw growth inhibition (reversal of dental bite) due to rapid orthognathic correction within a few months. Furlow's technique is a surgical procedure that reduces the risk of reversal of dental bite due to upper jaw growth inhibition in palatoplasty, but since it invades the upper jaw, it may slightly suppress the growth of the upper jaw to invade the upper jaw.
After presurgical nasoalveolar molding treatment and palatoplasty, orthodontic treatment, such as maxillary anterior traction, is performed (to adjust dental bite and dentition).
Advantages of less frequent surgeries
Treatment that is combined with presurgical nasoalveolar molding treatment, which may require only one surgery, can reduce medical costs compared with conventional surgical and hospitalization expenses. Generally, at least four surgeries and hospitalization are required: plastic surgery of lip, palatoplasty, alveolar bone grafting, and nasal revision surgery. The total cost of four surgeries will be approximately 1,150,000 to 1,480,000 yen, and it will increase further factoring in the cost of hospitalization.
On the other hand, the operative cost for a single surgery is approximately 740,000 yen, with only one hospitalization required. In addition, it will further reduce the burden on the patient, taking into account not only the patient but also the mental and transportation costs of the patient's family.
Surgeries are not necessarily completed only in one session, but we believe that reducing the number of surgeries has a beneficial effect on Japan's medical economy.
Speech and Language Assessment Results after Palatoplasty with Furlow's Technique
The speech and language assessment results (ages at the assessment: 5 years and 7 months ± 15 months) of 78 patients with unilateral cleft lip and cleft palate who underwent surgery at our Center for 5 years from 2010 to 2015 are as follows:
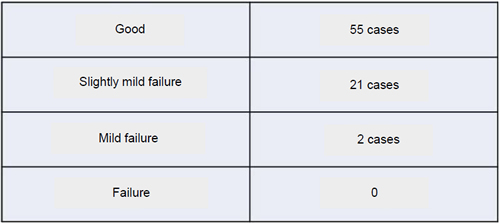
Annual Report of Kanagawa Children's Medical Center, Kanagawa Prefectural Hospital
Organization, 2010 N041-2014 N045
In general, patients with "good" and "slightly mild failure" in the speech and language assessments have no inconvenience in terms of language use in daily life, but patients with mild failure and failure need additional surgeries. Two of the 78 patients underwent additional surgery to improve their language use. These two patients had a cleft palate greater than 10 mm. A wide cleft palate makes surgery difficult.
Cases of Cleft Lip and Cleft Palate and Treatment Progresses
Cleft lip and cleft palate – treatment progresses
Types of cleft lip and cleft palate
Cleft lip and cleft palate are basically classified as cleft lip, cleft lip and alveolus, cleft of lip, jaw and cleft palate, and cleft palate.
Cleft lip and cleft palate on the right side
Cleft lip and cleft palate is the splitting of the lip from the upper lip beyond the upper jaw to the uvula.
Before surgery/After surgery (11 years old)

Left: At first visit before presurgical nasoalveolar molding treatment/Right: At age 11
This is a patient with unilateral cleft lip and cleft palate, where a split is on one side of the upper lip, and the upper jaw is split on one side. There was a cleft lip and cleft palate on the right side, and presurgical nasoalveolar molding treatment was performed to align the jaw, followed by plasty of lip, jaw, and cleft palate.
This patient has good speech and dental bite, but because of the deformity of the nose, we are planning to perform a nasal revision surgery at the end of growth. Only one surgery has been performed so far.
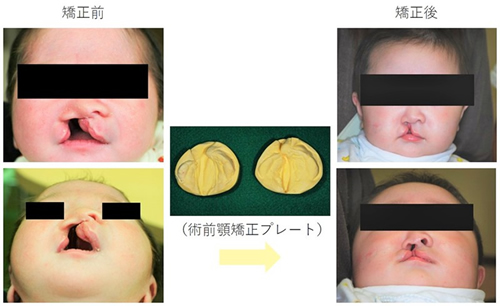
Left: Before presurgical nasoalveolar molding treatment
Middle: Presurgical nasoalveolar molding plates
Right: After presurgical nasoalveolar molding treatment
This is a patient with unilateral cleft of lip, jaw and cleft palate, where the upper lip and jaw are split on one side. The jaw was aligned using presurgical nasoalveolar molding plates because of the cleft of lip, jaw and cleft palate on the right. At the end of the presurgical nasoalveolar molding treatment, the cleft in the upper jaw was narrowed.
At age 11

After plasty of lip, jaw, and cleft palate, at age 11
The patient underwent lip, jaw, and cleft palate plasty, speaks well, and has a good dental bite at age 11. We are planning a nasal revision surgery at the end of growth because of the deformity of the nose. Only one surgery has been performed so far.
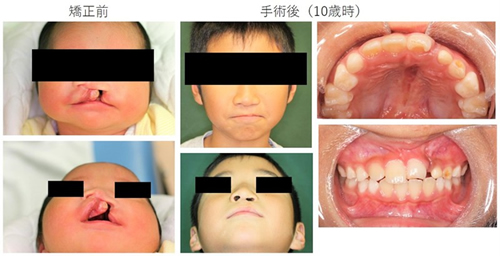
Cleft lip and cleft palate on the left side
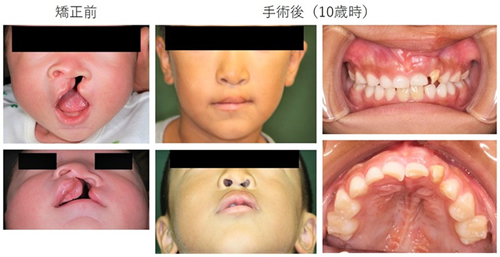
Left: At first visit before presurgical nasoalveolar molding treatment
Right: At age 10
This is a patient with unilateral cleft of lip, jaw and cleft palate, where the upper lip and upper jaw are split on one side. There was a cleft of the lip, jaw and palate on the left side, and presurgical nasoalveolar molding treatment was performed to align the jaw, followed by plasty of lip, jaw, and cleft palate. This patient has good speech and dental bite at age 10, but we are planning a nasal revision surgery at the end of growth because of the deformity of the nose. Only one surgery has been performed so far.
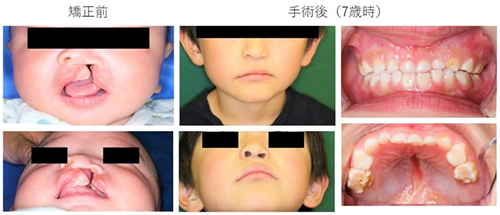
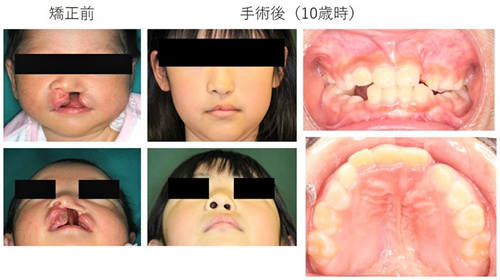
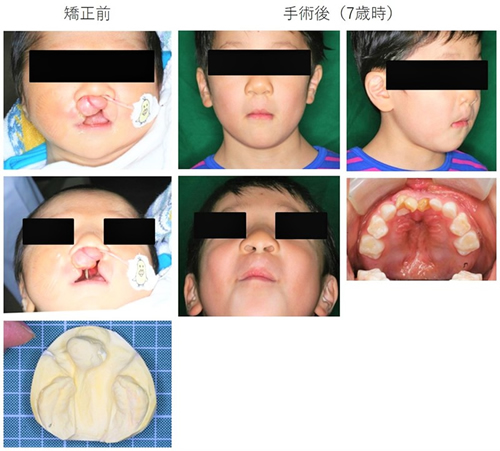
Left: At first visit before presurgical nasoalveolar molding treatment
Right: At age 7
This is a patient with unilateral cleft of lip, jaw and cleft palate, where the upper lip and upper jaw are split on one side. There was a cleft of lip, jaw and cleft palate on the left side, and presurgical nasoalveolar molding treatment was performed to align the jaw, followed by plasty of lip, jaw, and cleft palate. This patient has good speech and dental bite at age 10, but we are planning a nasal revision surgery at the end of growth because of the deformity of the nose. Only one surgery has been performed so far.
Left: At first visit before presurgical nasoalveolar molding treatment
Right: At age 10
This is a patient with unilateral cleft of lip, jaw and cleft palate, where the upper lip and upper jaw are split on one side. There was a cleft of lip, jaw and cleft palate on the left side, and presurgical nasoalveolar molding treatment was performed to align the jaw, followed by plasty of lip, jaw, and cleft palate. This patient has good speech and dental bite at age 10, but we are planning a nasal revision surgery at the end of growth because of the deformity of the nose. Only one surgery has been performed so far.

Left: At 6 months old, after completion of presurgical nasoalveolar molding treatment
Right: At age 10
This is a patient with unilateral cleft of lip, jaw and palate, where the upper lip and upper jaw are split on one side. Presurgical nasoalveolar molding treatment was performed to align the jaw, followed by plasty of lip, jaw and plate, then, cleft bone grafting at 6 years old. Two surgeries have been performed so far. This patient has good speech and dental bite at age 10, but we are planning a nasal revision surgery at the end of growth because of the deformity of the nose.
Left: At first visit before presurgical nasoalveolar molding treatment
Right: At age 10
This is a patient with unilateral cleft of lip, jaw and cleft palate, where the upper lip and upper jaw are split on one side. There was a cleft of lip, jaw and cleft palate on the left side, and presurgical nasoalveolar molding treatment was performed to align the jaw, followed by plasty of lip, jaw, and cleft palate. This patient has good speech and dental bite at age 10, but we are planning a nasal revision surgery at the end of growth because of the deformity of the nose. Only one surgery has been performed so far.
Complete bilateral cleft lip and alveolus
The condition where a split extends to the upper lip and to the jaw (gums) and the left and right skin and bones are separated is called "complete cleft lip and alveolus." Cases with splits in both sides are more difficult to treat than those with a split on one side.

Left: Before surgery
Right: At age 5
This is a patient with complete bilateral cleft of the lip and alveolus, where a split extends from the upper lip to the upper jaw. The split in the jaw is mild. One surgery has been performed so far.
Left: Before surgery
Right: After surgery at age 13, and treatment is continuing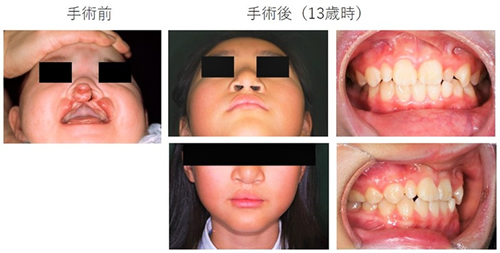
Left: Before surgery
Right: At age 13
This is a patient with complete bilateral cleft of the lip and alveolus, with splits in both sides of the lip. Because of the large protrusion seen between the splits (premaxilla), presurgical nasoalveolar molding treatment was performed to align the jaw, followed by lip plasty and GPP. This patient's postoperative shapes of nose and philtrum are good, but the nasal column is still a little shorter, so we need to continue treatment in the future.
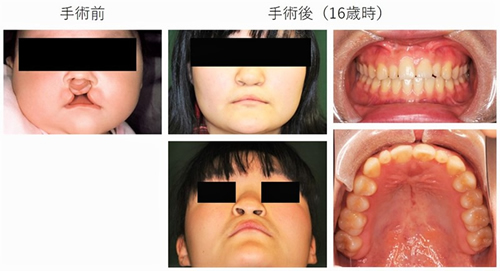
Left: Before surgery
Right: At age 16
This is a patient with complete bilateral cleft of lip and alveolus, where the split extends from the upper lip to the jaw. Because of the large protrusion of the premaxilla, presurgical nasoalveolar molding treatment was performed to align the jaw, followed by lip plasty and GPP. The patient is undergoing orthodontic treatment at the age of 16 years.
Complete bilateral cleft of lip, jaw and cleft palate
The condition where a split extends from the upper lip and the jaw (gums) to the uvula, and the left and right upper lips split is called a "complete cleft of lip, jaw and cleft palate." The bones from which the front teeth develop might bulge forward.
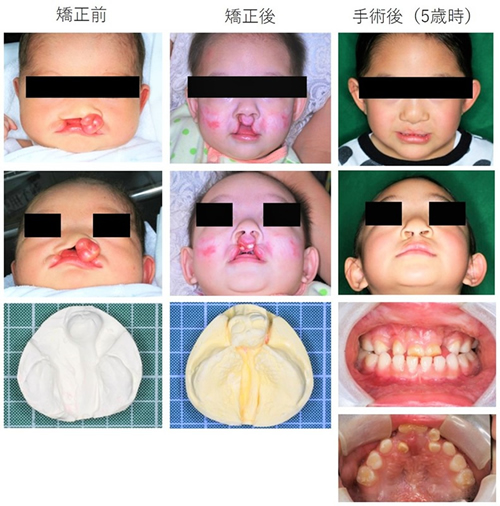
Left: Before presurgical nasoalveolar molding treatment
Middle: After completion of treatment using presurgical nasoalveolar molding plates
Right: At age 5
This is a patient with complete bilateral cleft of lip, jaw and cleft palate, where the upper lip and upper law are split on both sides. The bones in which the front teeth grow protrude and turn to the left. Presurgical nasoalveolar molding plates were used to align the jaw. At the end of presurgical nasoalveolar molding treatment, the cleft in the upper jaw was narrowed.
Plasty of lip, jaw and cleft palate was then performed. This patient has good speech and good facial appearance at age 5. Orthodontic treatment is planned for the future because of the disturbance in the alignment of the teeth. Only one surgery has been performed so far.
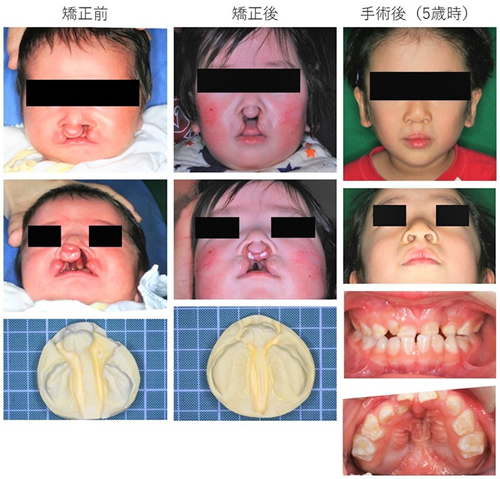
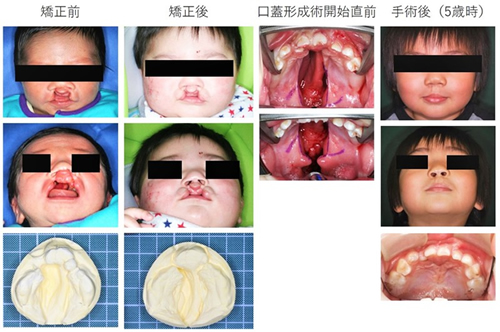
Left: Before the start of presurgical nasoalveolar molding treatment
Middle: After completion of treatment using presurgical nasoalveolar molding plates
Right: At age 5
This is a patient with complete bilateral cleft of lip, jaw and cleft palate, where the upper lip and upper law were split on both sides. Presurgical nasoalveolar molding plates were used to align the jaw. At the end of presurgical nasoalveolar molding treatment, the cleft in the upper jaw was narrowed.
Plasty of lip, jaw and cleft palate was then performed. This patient has good speech and good facial appearance at age 5. Orthodontic treatment is planned for the future because of the disturbance in the alignment of the teeth. Only one surgery has been performed so far.
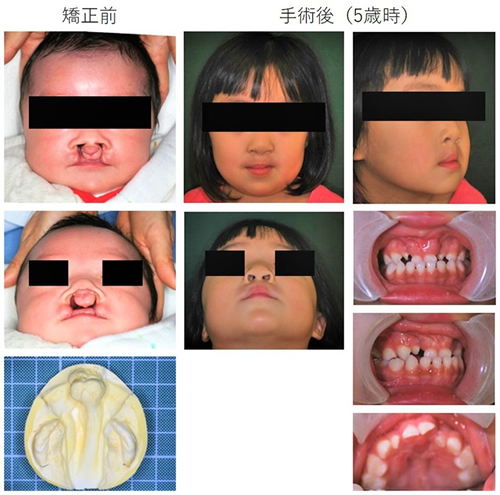
Left: Before the start of presurgical nasoalveolar molding treatment
Right: At age 5
A patient with complete bilateral cleft of lip, jaw and cleft palate, where the upper lip and upper law are split on both sides. Because the reaction to presurgical nasoalveolar molding plates was slow, we performed premaxillary osteotomy to cut the bone that was protruding forward, followed by surgery to lower the bone.
Palatoplasty was then performed. This patient has good speech and good facial appearance at age 5.
Orthodontic treatment is planned for the future because of the disturbance in the alignment of the teeth. Two surgeries have been performed so far.
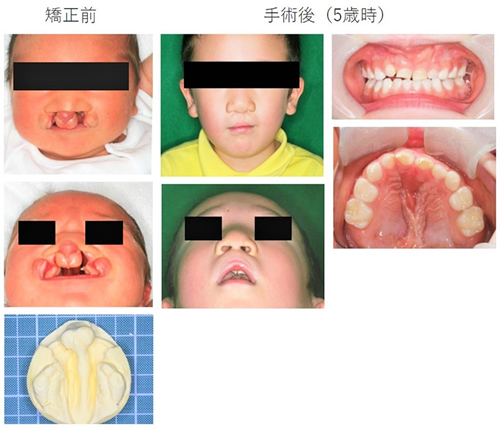
Left: Before the start of presurgical nasoalveolar molding orthognathic
Right: At age 5
A patient with complete bilateral cleft of lip, jaw and cleft palate, where the upper lip and upper jaw are split on both sides. Because the reaction to presurgical nasoalveolar molding plates was slow, we performed premaxillary osteotomy to cut the bone that was protruding forward, followed by surgery to lower the bone.
Palatoplasty was then performed. This patient has good speech and good facial appearance at age 5.
Orthodontic treatment is planned for the future because of the disturbance in the alignment of the teeth. Two surgeries have been performed so far.
Left: Before the start of presurgical nasoalveolar molding treatment
Right: At age 7
A patient with complete bilateral cleft of lip, jaw and cleft palate, where the upper lip and upper jaw are split on both sides. Because it was not possible to correct with presurgical nasoalveolar molding plates, we performed premaxillary osteotomy to cut the bone that was protruding forward at 6 months, followed palatoplasty.
This patient has good speech and good facial appearance at age 5. Since one anterior tooth is congenitally missing and other anterior teeth are hypoplastic and accompanied by irregular dentition, orthodontic treatment is planned for the future. Two surgeries have been performed so far.
Cleft lip and cleft palate
From the left, before the start of presurgical nasoalveolar molding treatment, at the end of treatment using presurgical nasoalveolar molding plates, immediately before the start of palatoplasty, and at age 5
This is a patient with complete bilateral cleft of lip, jaw and cleft palate, where the upper lip and upper jaw are split on both sides. Presurgical nasoalveolar molding plates were used to align the jaw. The cleft seen in the upper jaw was narrowed at the end of presurgical nasoalveolar molding treatment. Plasty of the lip and jaw was performed.
The patient then underwent palatoplasty at 18 months because of the wide cleft palate.
This patient has good speech and good facial appearance at age 5. Orthodontic treatment is planned for the future because of the disturbance in the alignment of the teeth. Two surgeries have been performed so far.
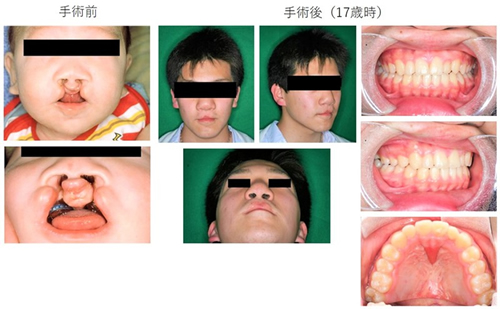
Left: Before surgery
Right: At age 17
This is a patient with complete bilateral cleft of lip, jaw and cleft palate, where the upper lip and upper jaw are split on both sides. Plasty of lip, jaw and cleft palate was performed. This patient has good speech and good face at age 17. Two surgeries have been performed: lip plasty with GPP and palatoplasty.
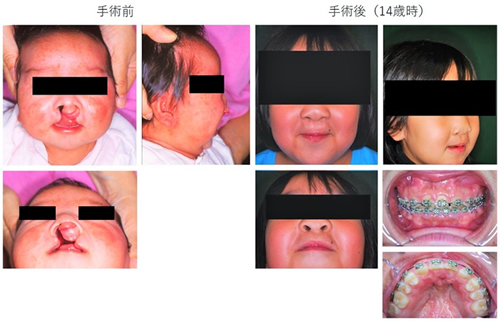
Left: Before surgery
Right: At age 14
This is a patient with complete bilateral cleft of lip, jaw and cleft palate, where the upper lip and upper jaw are split on both sides.
Plasty of lip, jaw, and cleft palate was performed. This patient has good speech and a good facial appearance at age 14. Orthodontic treatment is being performed to align dentition. A total of three surgeries have been performed: lip plasty with GPP, palatoplasty, and cleft bone grafting.
Closing remarks by the doctor
An elementary school student
Courtesy of Payless images
When a child is found to have a cleft lip and cleft palate, the parents feel very anxious and worried. However, many children with a cleft lip and/or cleft palate can, provided it does not affect their brain development and they receive appropriate treatment at the appropriate time, live in the same manner as healthy children. In most cases, social activities, such as going to school, getting married, or having children, are not affected.
If a prenatal diagnosis suggests that the baby may have cleft lip and/or cleft palate, take advantage of the diagnosis and consult with a hospital to receive the necessary care and support. In our hospital, medical staff and certified genetic counselors work together to provide adequate support.